Atenolol
Severe
Textbook-cited
Enhanced bradycardia and hypotension.
Avoid concurrent use
Source: KDT 7e · p950
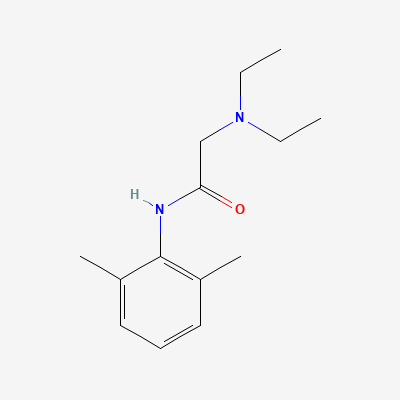
Local Anesthetic
Also known as Lidocaine hydrochloride
KDIGO 2024 + manufacturer label
106 branded formulations and 223 fixed-dose combinations. Look up specific brands in the Drugs workspace.
Lidocaine is a class IB antiarrhythmic and amide-type local anesthetic. As an antiarrhythmic, it blocks voltage-gated sodium channels in their open or inactivated state, preferentially affecting ischemic or depolarized tissues (such as in myocardial infarction). It shortens the action potential duration and effective refractory period in Purkinje fibers and ventricular muscle, and suppresses automaticity in ectopic foci. As a local anesthetic, it blocks sodium channels in neuronal membranes, preventing depolarization and propagation of action potentials, resulting in reversible loss of sensation in the targeted area. Unlike ester-type local anesthetics, lidocaine is metabolized by hepatic amidases and does not require plasma pseudocholinesterase.
FDA PLLR: Animal studies showed no teratogenicity. Widely used in pregnancy for local anesthesia. Large doses may cause fetal bradycardia. Use lowest effective dose.
Excreted in breast milk in low concentrations. Compatible with breastfeeding for local anesthesia. Monitor infant if large systemic doses used.
Enhanced bradycardia and hypotension.
Avoid concurrent use
Source: KDT 7e · p950
Enhanced bradycardia and hypotension.
Avoid concurrent use
Source: KDT 7e · p950
Enhanced bradycardia and hypotension.
Avoid concurrent use
Source: KDT 7e · p950
Enhanced bradycardia and hypotension.
Avoid concurrent use
Source: KDT 7e · p950
Exaggerated cardiac depression; may precipitate arrhythmias
Avoid concurrent use
Source: KDT 7e · p950
Drug interaction classified as: metabolism
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Drug interaction classified as: synergy.
Source: DDInter
Drug interaction classified as: metabolism
Source: DDInter
Clinical effect not specified
Source: DDInter
Clinical effect not specified
Source: DDInter
.
Source: DDInter
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: KD Tripathi 7e, Goodman & Gilman 14e, Harrison 22e, Katzung·Verified: 2026-05-18 · House clinical team·Cockpit curated: 2026-05-18