Aspirin
Severe
Textbook-cited
Significantly increased GI bleeding risk.
Concurrent use is contraindicated; if unavoidable, add PPI
Source: KDT 7e · p950
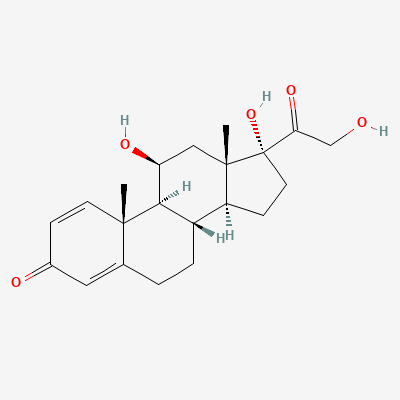
Corticosteroid
Also known as Prednisolone acetate, Prednisolone sodium phosphate, Delta-1-cortisol, Metacortandracin
KDIGO 2024 + manufacturer label
Prednisolone, a synthetic glucocorticoid, exerts its effects by binding to intracellular glucocorticoid receptors. This binding leads to translocation of the receptor-ligand complex into the nucleus, where it modulates gene expression. It upregulates anti-inflammatory proteins and downregulates pro-inflammatory mediators, thereby reducing inflammation and immune responses. It also inhibits phospholipase A2, reducing prostaglandin and leukotriene synthesis.
Category C — placental 11β-HSD2 protects fetus; mostly safe
Prednisolone is excreted into breast milk. While generally considered safe at usual therapeutic doses, infants should be monitored for signs of adrenal suppression or growth abnormalities. For high doses, a brief interruption of breastfeeding (e.g., 3-4 hours after the dose) may be considered.
Significantly increased GI bleeding risk.
Concurrent use is contraindicated; if unavoidable, add PPI
Source: KDT 7e · p950
Significantly increased GI bleeding risk.
Concurrent use is contraindicated; if unavoidable, add PPI
Source: KDT 7e · p950
Significantly increased GI bleeding risk.
Concurrent use is contraindicated; if unavoidable, add PPI
Source: KDT 7e · p950
Significantly increased GI bleeding risk.
Concurrent use is contraindicated; if unavoidable, add PPI
Source: KDT 7e · p950
Significantly increased GI bleeding risk.
Concurrent use is contraindicated; if unavoidable, add PPI
Source: KDT 7e · p950
Significantly increased GI bleeding risk.
Concurrent use is contraindicated; if unavoidable, add PPI
Source: KDT 7e · p950
Significantly increased GI bleeding risk
Concurrent use is contraindicated; if unavoidable, add PPI
Source: KDT 7e · p950
Significantly increased GI bleeding risk.
Concurrent use is contraindicated; if unavoidable, add PPI
Source: KDT 7e · p950
Significantly increased GI bleeding risk
Concurrent use is contraindicated; if unavoidable, add PPI
Source: KDT 7e · p950
Drug interaction classified as: synergy.
Source: DDInter
Drug interaction classified as: others
Source: DDInter
Drug interaction classified as: synergy
Source: DDInter
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: KD Tripathi 7e, Goodman & Gilman 14e, Katzung, BNF·Verified: 2026-05-17 · House clinical team·Cockpit curated: 2026-05-16