Linezolid
Contraindicated
Database
Serotonin syndrome: hyperthermia, rigidity, myoclonus, mental status changes.
Do not combine. Stop SSRI 2 weeks before linezolid or use alternative antibiotic.
Source: DDInter
SSRI · Antidepressant
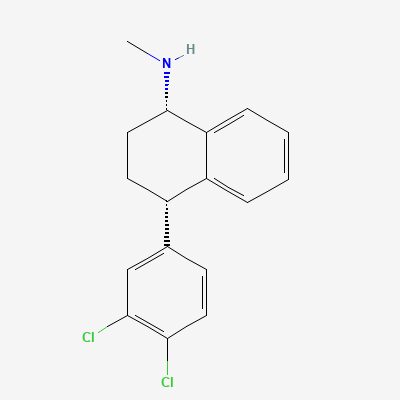
Also known as Sertraline hydrochloride, Zoloft, Lustral, Seralin
KDIGO 2024 + manufacturer label
327 branded formulations and 60 fixed-dose combinations. Look up specific brands in the Drugs workspace.
Jan Aushadhi — generic available at GoI pharmacies
Sertraline selectively inhibits the reuptake of serotonin (5-hydroxytryptamine, 5-HT) into presynaptic neurons in the central nervous system. This action leads to an increased concentration of serotonin in the synaptic cleft, enhancing serotonergic neurotransmission. Chronic administration results in downstream adaptive changes, including desensitization of postsynaptic serotonin receptors, contributing to its therapeutic effects.
Category C — most reproductive safety data; preferred SSRI in pregnancy
Sertraline is excreted into breast milk in small amounts. It is generally considered compatible with breastfeeding, especially at lower doses, but caution is advised. Monitor breastfed infants for potential adverse effects such as sedation, irritability, poor feeding, or changes in weight gain. Consult a physician before use during lactation.
Serotonin syndrome: hyperthermia, rigidity, myoclonus, mental status changes.
Do not combine. Stop SSRI 2 weeks before linezolid or use alternative antibiotic.
Source: DDInter
Serotonin syndrome (hyperthermia, rigidity, myoclonus, autonomic instability, mental status changes)
Sertraline is contraindicated with MAOIs. A washout period of at least 14 days is required between discontinuing an MAOI and starting sertraline, and at least 14 days between discontinuing sertraline and starting an MAOI.
Serotonin syndrome: agitation, hyperthermia, rigidity, seizures, potentially fatal
Contraindicated. Allow 14-day washout between SSRI and MAOI
Source: DDInter
Increased risk of QT prolongation and cardiac arrhythmias (e.g., Torsades de Pointes)
Concomitant use is contraindicated. Sertraline significantly increases pimozide exposure.
Source: DDInter
Increased risk of gastrointestinal bleed.
Monitor for bleeding; consider gastroprotective agents or alternative analgesics.
Source: KDT 7e
Increased risk of gastrointestinal bleed.
Monitor for bleeding; consider gastroprotective agents or alternative analgesics.
Source: KDT 7e
Increased risk of gastrointestinal bleed.
Monitor for bleeding; consider gastroprotective agents or alternative analgesics.
Source: KDT 7e
Increased risk of gastrointestinal bleed.
Monitor for bleeding; consider gastroprotective agents or alternative analgesics.
Source: KDT 7e
Increased risk of gastrointestinal bleed.
Monitor for bleeding; consider gastroprotective agents or alternative analgesics.
Source: KDT 7e
Increased risk of gastrointestinal bleed.
Monitor for bleeding; consider gastroprotective agents or alternative analgesics.
Source: KDT 7e
Increased risk of gastrointestinal bleed.
Monitor for bleeding; consider gastroprotective agents or alternative analgesics.
Source: KDT 7e
Increased risk of gastrointestinal bleed.
Monitor for bleeding; consider gastroprotective agents or alternative analgesics.
Source: KDT 7e
Continue into a citation-backed clinical answer with the drug context already attached.
Sources: Goodman & Gilman 14e, Harrison 22e, Katzung, BNF·Verified: 2026-05-16 · House clinical team·Cockpit curated: 2026-05-16